


The Covid Big Picture So Far: Part 2, Responding to Covid with Public Health Policy
We still need a public health response to the pandemic. Thoughts & links to scientific research on response including masking, ventilation, vaccines, & more -- a "Vaccines-Plus" strategy.
This essay is Part 2 of a series on Covid and will discuss the larger public health policy response and demands we need to organize around (such as universal healthcare!). Part 1 focused on what we’ve learned so far (as of December 2022) about Covid from science — very important to share today as most media and organizations and political figures continue to downplay the severity of Covid and “Long Covid”. Part 3 will look at lessons from this pandemic on organizing for climate change and other global issues.
Clean Air Is Key
In the previous Part 1, many scientific research articles were linked, describing Covid and “Long Covid” to better understand the disease and how it transmits. It’s worth a full read when you have time, but the major points for today’s discussion include:
Covid is a severe cardiovascular disease that attacks potentially any organ, including lungs, heart, and brain, and increasingly seems to harm the immune system itself, leaving many more susceptible to future infections. Covid is NOT “just a cold” and still far deadlier than the flu.
The organ damage caused by Covid can lead to “Long Covid”, a chronic illness in which patients face elevated risk for heart attack and other serious symptoms long after the initial infection, even if it was “mild”.
The organ damage is cumulative, meaning every time you get infected with Covid, the risk of developing serious complications like Long Covid increases. Just because you’ve had a “mild” case in the past does NOT mean you won’t develop a serious case or lingering issues next time.
Covid is airborne, and spreads primarily through the air in an aerosolized form (your breath or cough mists saliva containing Covid virus into the air, basically). Even people not feeling symptoms can spread Covid. This makes clean air and well-ventilated spaces key to stopping transmission and making workplaces and public spaces safer.
We’re facing a mass disabling event — literally millions of Americans, many of them children, are facing some kind of Long Covid complications, sometimes very serious, and we are setting ourselves up for heart, brain, and other issues over the next decade if we do not act quickly to control transmission as much as possible NOW.
So, let’s start talking about how to control the pandemic by talking about the air.
Masking — N95 or Better!
The easiest and cheapest way to protect yourself and others from aerosol transmission is to wear a face mask. Covid largely spreads by aerosol — meaning that Covid is largely AIRBORNE. The effectiveness of masking is confirmed both by models of aerosol transmission and real-world studies. Schools which require students and staff to wear masks have significantly lower transmission and infection rates than schools without a masking requirement. Mask mandates in schools were so effective at preventing transmission that it lessened the number of students and staff that needed to take time off, preventing schools from needing to shutdown due to being understaffed. Conversely, research also shows that once universal masking policies are lifted, cases dramatically rise.
What kind of mask should you wear? N95 respirators are common at any hardware store and often recommended when doing things like sanding down a wood floor that kick up small particles into the air; you wear the mask so you’re not breathing those particles into your lungs. Same concept, but with Covid-laced droplets. Research has shown that N95 respirators are extremely effective at preventing exposure to the Covid virus in particular, but really any kind of respiratory virus; N95s are far superior to surgical or cloth mask and so are recommended for most people. In fact, recent research showed that N95 respirators reduced infections by 40% in medical workers with regular exposure to the virus, and N95 respirators were superior to surgical masks in a dentist setting. For even greater protection, N100 and P100 masks are also available at hardware stores but they are more expensive and may need special filters replaced frequently, but increase the protection further. None of this should be particularly surprising as masking has been shown effective for decades to protect workers from airborne particles, virus-laden aerosols or not.
With clear proof and relatively cheap costs, it is therefore vital that schools and other public places reinstate masking requirements. It also underscores the failure of the Biden administration to respond to this pandemic, since most cities are still parroting the Biden administration’s talking point that the economy is “open” and so have no plans to reinstate a mask mandate. Masks should have been mass produced and distributed for free as part of a broader response; we can and should still distribute them today to ensure everyone has a steady supply of clean masks/PPE. National Nurses United, the largest union of nurses in the country, is advocating OSHA Covid standards that would at least ensure hospitals and medical facilities retain masking mandates beyond federal emergency requirements, but many more public locations should also be looking at masking rules — grocery stores and other essential places, for example. Recent journal articles also called for “permanently including universal masking in routine patient-care interactions” in all healthcare settings, showing growing momentum among health professionals for masking in healthcare settings.


Unfortunately, in late February 2023, a Cochrane report concluded that masking was not very effective, prompting many in government and media to argue against the need for masks or masking mandates, even in cases with higher transmission risks like hospitals. This report however compared “apples to oranges”, and mixed up different studies that were in very different conditions — not all of the studies cited in the report were even about Covid, but instead looked at masking for other viruses like influenza! The important point to keep in mind is that this Cochrane report is extremely flawed and shouldn’t be used to draw conclusions or make policy; good scientific studies so far, as outlined above, show that masking particularly with N95 or better respirators DOES provide very good protection from Covid.
Outdoor Spaces
It is important to note quick that you can catch Covid outdoors. Covid is a particularly transmissible virus, far more than most others, so it can be caught even outdoors in short exposure. Even if outdoors, if you are at a crowded event, it is a good idea to still wear a high-quality mask. Organizations hosting events should consider masking requirements even if the event is outdoors.
Air Filtration and Improved Ventilation
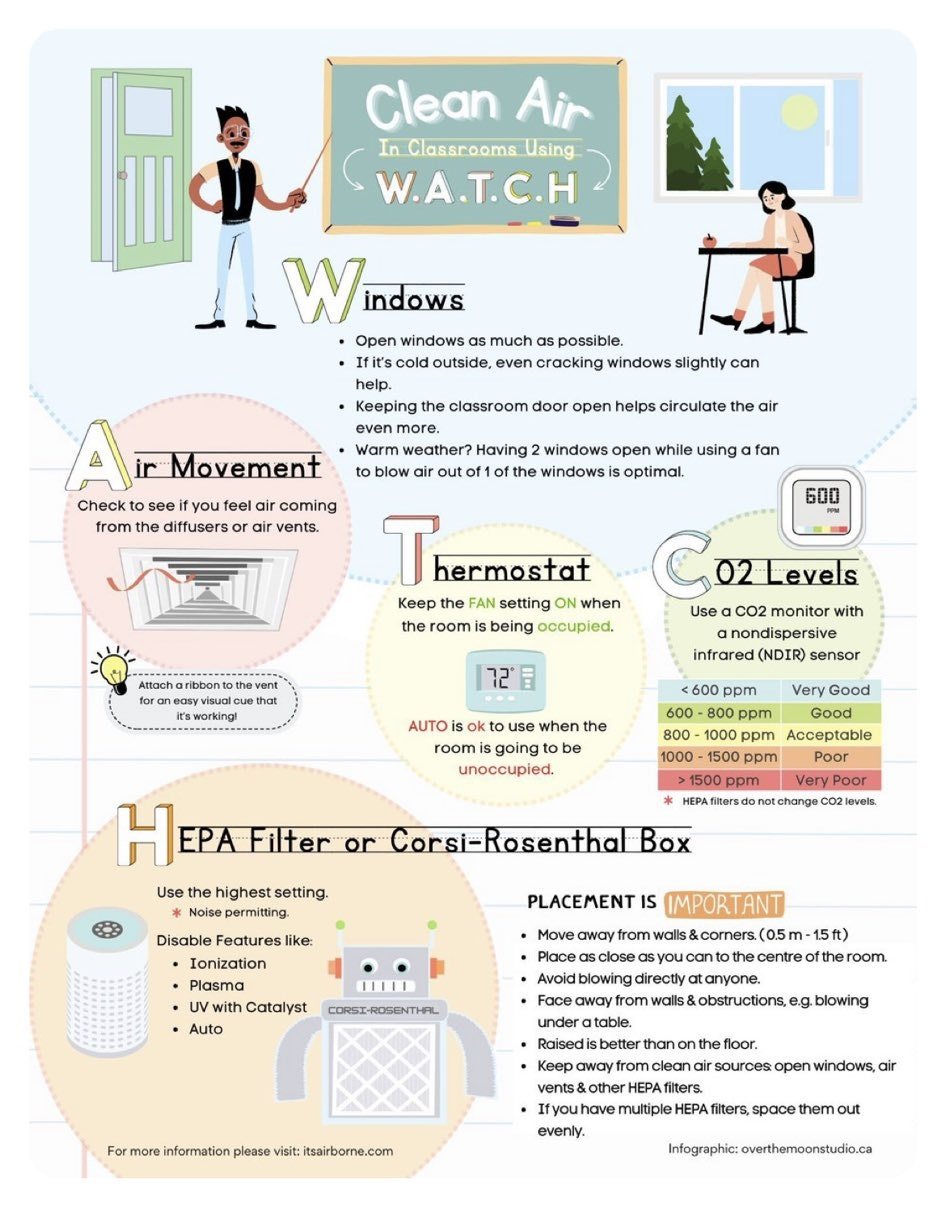
Masking is something individuals can do, however individuals cannot choose the air quality indoors and in public spaces. In this case, business and government must take precautions to improve ventilation and filtering of the air in these public-facing spaces to minimize aerosol transmission of the virus through the air. HEPA filters have been shown scientifically to dramatically reduce the number of viruses in the air. A March 2023 study showed that “97-99%” of coronavirus particles could be filtered from the air via HEPA filters. A July 2024 study from Harvard also showed that portable air filters can reduce aerosol intake by up to 66%. “Fancy” filters aren’t needed; conventional HEPA filters can continuously remove viruses from the air. “Brand names” may be expensive but Corsi-Rosenthal boxes can be built cheaply out of large furnace filters and fans to be nearly as effective; peer-reivewed studies have even shown that Corsi-Rosenthal MERV-13 boxes can be more effective than HEPA.
Ventilation can be improved even by simply opening windows, but many larger buildings will likely need updated HVAC systems to mechanically force air ventilation. One way to measure if ventilation is adequate is to measure CO2 — since people breathe in oxygen and breathe out CO2, CO2 will build up in indoor spaces without ventilation. It is generally accepted that a CO2 concentration under 800 ppm (parts-per-million) is adequate and can reduce the risk of transmission; France is now requiring schools to monitor CO2 and take action when above 800ppm and immediate action when above 1500ppm. Similar rules in the US should be implemented; California is first to start adopting workplace health and safety rules for Covid, and Utah is considering funding air filtration in every classroom, but we need much more and nationwide. The People’s CDC provides some tips on CO2 monitoring to determine if the ventilation in a space is adequate.
What sort of standards should workers organize around for workplace safety? There are several professional societies providing recommendations that workers should pick up.
The American Society of Heating, Refrigerating and Air-Conditioning Engineers (ASHRAE) “is a global professional society of over 55,000 members committed to serve humanity by advancing the arts and sciences of heating, ventilation, air conditioning, refrigeration and their allied fields” according to their website; ASHRAE has COVID guidelines for re-opening buildings which are recommended by OSHA and the CDC. (In fact, OSHA advises that employees are protected from “discrimination” or “retaliation” by employers for asking about and requesting workplace protections such as improved ventilation against Covid.) The American Industrial Hygiene Association (AIHA) and the American Conference of Governmental Industrial Hygienists (ACGIH) both say that at least 6 ACH (air changes per hour, a measurement of how much ventilation and filtration is present in a space) is needed to control bioaerosols that spread viruses, which is in line with the ASHRAE recommendation of 6-12 ACH depending on circumstances.
The People’s CDC, “a coalition of public health practitioners, scientists, healthcare workers, educators, advocates and people from all walks of life working to reduce the harmful impacts of COVID-19” according to its website, provides some ventilation guidelines that endorse ASHRAE standards.
The Lancet, “an independent, international weekly general medical journal founded in 1823 by Thomas Wakley”, created a Lancet COVID-19 Commission that has published recommendations on air ventilation and filtration that also draw from ASHRAE. There is clear growing consensus among experts that ventilation and filtration are needed to truly end the pandemic.
States like Illinois are funding HEPA filtration in schools. We should push on local, state, and federal to fund ventilation and filtration in schools and public spaces, and require workplaces to take action.
Ultraviolet light systems
Another layer of defense in addition to filtration and ventilation is the use of ultraviolet (UV) light systems to disinfect the air. UV light from the sun can be dangerous and cause burns and skin cancer, but this is largely because of specific high-energy forms of UV light that can penetrate your skin and eyes to cause damage. Studies suggest far UV-C light does not do this and is safe for long-term use while remaining highly effective at cleaning bacteria and viruses. Public spaces such as schools should consider adoption of these systems to mitigate pandemic risk. Some schools such as in Franklin, Massachussetts, have already adopted UV ligh systems.
Ultimately, all of the above — ventilation, filtration, and UV light systems — help minimize transmission by cleaning the virus directly out of the air before anyone is exposed to it. Minimizing transmission is important and our first line of defense, but what to do if you catch it anyway?
Regular Testing and Quarantining
Testing should be part of a public response as well, as it can help keep statistics on which areas are facing surges and need additional resources. Unfortunately, with most mass testing locations winding down, at-home tests are not providing good data and statistics and likely to be vastly undercounting infections. Considering that infection rates remain high across the country even with this undercounting, it is important to keep taking precautions and test yourself whenever you may have been exposed to the virus, even if you don’t yet feel symptoms.
If you do feel symptoms or test positive, try to isolate yourself and get medical advice from a doctor if you have been exposed. While the Biden CDC suggests 5 days of quarantine is enough, scientific data suggests that 10 days should be the guideline. The FDA recommends testing at least three times spread out over a few days when using the home rapid tests.
If you test positive, it is important to take care of yourself and take action to prevent transmitting to others. The American Lung Association for example recommends staying home, ensuring you stay hydrated and getting plenty of rest, monitoring for symptoms that may show signs of more seriousness illness such as trouble breathing (in which case you should go to the nearest emergency room for testing/treatment). It is recommended to avoid going to public places or work or school until you’ve not had fever for at least 24 hours (and consider the 5-10 day quarantine guideline discussed above) — and even when you do go back into public, wear a high-quality N95 mask or better!
Of course, folks have to pay bills and that often means needing to work jobs even if sick. Early in the pandemic, quarantines and “lockdowns” were used to prevent transmission; studies show that such lockdowns are very effective at dramatically reducing transmission but of course such actions are difficult to maintain for several reasons including workers’ needing economic aid to pay the bills while staying home. We’ll come back to this point later in the essay.
Ideally, your body’s immune system would fight it off before it became a major infection or caused damage. The best way to prime your immune system is to get a vaccine, so let’s talk vaccines next.
Covid Vaccines and Boosters
Vaccines work essentially by introducing your body to a “fake” infection so that your body builds the defenses necessary to fight the illness if you were to get a “real” infection later on. Unvaccinated people are eight times more likely to develop serious Covid illness than folks that received both doses of the original vaccine. According to another study, “In conclusion, even in patients with severe COVID-19, vaccination mitigates the probability of long COVID symptoms.” Recent research also shows vaccination lowers the odds of heart attack and stroke after a Covid infection. Even as of January 2024, new studies confirms that vaccination reduces risk of severe symptoms and long Covid. In summary studies show the vaccines provide strong, if not perfect, protection that significantly reduces your chances of severe illness or Long Covid.
Several different Covid vaccines are available to be up-to-date — this means getting a “booster”, not just the initial 2 doses that the Biden administration is misleadingly calling “fully vaccinated”. A new bivalent booster — meaning it covers both the original variants of Covid plus some of the newer Omicron variants — is now available, and is highly recommended for everyone of all age ranges, even if you’ve had the initial 2 doses and a booster. You can find pharmacies and locations near you that provide the bivalent booster online. Research has shown that the bivalent booster is very effective at preventing serious illness, especially for adults under 50 — this makes the bivalent booster important for all young adults and workers under 50. However, it must be noted that some pre-print (not yet peer reviewed and published) raises concerns that the bivalent booster may not be clearly effective against the new XBB variants of Covid that are becoming prevalent as of April 2023, so that updated vaccines may be needed to maintain maximum effectiveness.
These vaccines, particularly those based on mRNA, have been misunderstood due to misinformation about them. A short, not comprehensive list of misinformation and rumors about Covid vaccines, and answers to those concerns, is below:
CLAIM: Vaccines are “untested” or “experimental”.
FACTS: This largely stems from the “emergency authorization” for the vaccines at the start of the pandemic in December 2020. Emergency authorization does not mean the vaccines weren’t tested; they were still required to meet the same high standards in clinical trials. All of this is moot now, as the original Pfizer and Moderna vaccines have now received full authorization; Pfizer as of August 2021, and Moderna as of January 2022. Additionally, Novavax was given emergency authorization as of October 2022 and expecting full approval soon, which gives patients a “traditional” vaccine alternative to mRNA vaccines if there is any concern. The FDA website has further links to studies and reports required to receive authorization, emergency or not.CLAIM: Vaccines are causing myocarditis or heart problems in children (or even young adults).
FACTS: Studies have shown that Covid itself causes myocarditis. This claim is misunderstanding risks; children are far less likely to develop myocarditis after getting vaccinated than remaining unvaccinated. Since 2020, we’ve known that Covid is linked to higher risk of stroke even in otherwise healthy young adults, leading many experts at the time — before vaccines were even available! — to become concerned about Covid causing heart attacks in athletes, something we are seeing more and more today as society has gone “back to normal” and halted all mitigations. With Covid spreading uncontrolled at this point, children & young adults are far safer being vaccinated than left unvaccinated to fight a Covid infection.CLAIM: The Covid virus is not serious or “just a cold” and it is the vaccines causing heart problems and other complications.
FACTS: Studies show that Covid does indeed cause serious cardiovascular problems including strokes and heart attacks, even in people that seem otherwise healthy before being infected with Covid. In April 2023, new research has not found any association between vaccination and heart attacks. These studies tracked vaccinated individuals and show that the cardiovascular damage is clearly coming from Covid infections, not vaccines.CLAIM: OK, fine, traditional vaccines like Novavax might be ok, but mRNA is causing complications.
FACTS: In addition to studies mentioned above, a March 2023 study showed that mRNA vaccines had no correlation to any complications. The complications are however strongly correlated with Covid infections, especially if you haven’t been vaccinated. So this is additional very strong evidence that the mRNA vaccines are safe and effective.CLAIM: Vaccines are causing or worsening mutation of Covid.
FACTS: Studies have shown increases in Covid are unrelated to levels of vaccination. Covid continues to mutate and spread not because of folks being vaccinated, but because we are not slowing transmission among a population that is still not widely up-to-date on vaccines: one third of Americans haven’t even received the original two-dose vaccine, and two thirds of Americans haven’t received a booster.CLAIM: Immunity from infection is “just as good” so don’t need vaccines.
FACTS: This misunderstands the purpose of vaccines, which is to gain immunity without being infected first and risking serious disease or death. This claim is going around more recently after research showed that immunity from infection is about the same as vaccine. Some quick responses to misinterpretations of this study: (1) it was conducted on the early variants & original vaccine, so may not apply to the new Omicron variants & new bivalent booster; (2) the immunity from infection still wanes over time, so unless you plan to get reinfected & risk serious disease again every 6 months to a year indefinitely into the future (remember that research also shows the damage to your body increases chances of severe disease every time you catch Covid! so the odds get worse each time), we’re still going to need boosters; (3) again, remember, the point of the vaccine is to protect you from serious disease; the study only looked at the immunity after infection, and does not address the chances and risks of severe disease, “Long Covid”, or death from infection before immunities are formed. It is far better to get the vaccine to protect yourself from serious disease and Long Covid! You don’t develop immunities if you die from Covid infection first. And, with Omicron subvariants spreading, there is evidence that newer subvariants of Omicron are escaping immunities from past infection, so relying only on infection won’t necessarily prevent future infections (so you’ll end up sick multiple times and possibly with long-term symptoms).
Whichever Covid vaccine is used, all have been shown to be very safe and effective, significantly lowering risk of severe illness. Unvaccinated children are far more likely to have serious complications. “Excess deaths”, which is a measure of how many unexpected deaths have occurred as a result of the pandemic compared to typical years, spiked in counties with low vaccination rates and along partisan lines (with Republicans less likely to be vaccinated than Democrats). This difference in excess deaths only occurs in the data after the vaccine was made available — in other words, once vaccines were available, the excess deaths dropped significantly in counties and populations that got vaccinated, showing strong evidence that the vaccines have been effective in preventing death and serious outcomes.
Research shows the vaccines also benefit those around you. Studies have shown being vaccinated reduces your viral load — “vaccinated individuals are less infectious than unvaccinated individuals”. Recent research also shows that getting boosters reduces transmission even more. Conversely, recent research shows that large unvaccinated populations “markedly” increased virus transmission and infection, affecting even those that are vaccinated as the virus mutates around immunities (whether from vaccination or prior infection). Scientific studies estimate nearly 20 million lives have been saved in the first year of vaccines being available alone. Therefore, in addition to wearing masks and filtering the air, getting vaccinated and boosted provides additional protection not only to yourself but those around you.
A Brief Word on Vaccine Requirements
For these reasons, vaccine requirements (or “mandates”) may be good policy for some workplaces that are particularly at risk — hospitals and care facilities like nursing homes especially, where patients are at substantial risk of transmission and need extra protection. A multi-society statement put out by 50+ professional medical organizations related to infectious diseases called for support of mandates in hospitals, and many hospitals including Mayo Clinic have gone on to enforce employee mandates in medical facilities based on the science showing it is effective and important for protecting both employees and patients. Schools have also had historical vaccine requirements (such as here in Pennsylvania) that were critical for ending polio and other diseases; the decision lies with states and school districts themselves, so districts could decide to set requirements if it makes sense based on local conditions. It is important to defend vaccine requirements from right-wing attacks that feed anti-vaccine fervor against not only Covid vaccines but all vaccines, which has been leading to outbreaks of measles, polio, and other diseases. It is also important to understand that health and religious/philosophical exemptions exist in all states; the goal isn’t to “force” everyone (certainly not “at gunpoint” / with violence, as is usually implied) but to set a high expectation to get vaccinated or otherwise work together with employees, employers, and communities, to set alternative accommodations that keep everyone safe. In usual circumstances, the exemptions meant being willing to stay home during disease outbreaks, but since Covid is on-going and showing no signs of ending, we will need to ensure better accommodations continue to exist, such as but not limited to additional requirements for masking, air filtration, regular testing, and virtual attendance / work-from-home options, as appropriate.
Exactly what accommodations look like depends on the job, workplace conditions, etc., but the important thing is that public safety is emphasized while workers & families are not left behind. Unfortunately, economic rights were not respected in many workplaces and even government offices, leaving many workers to wonder about their jobs and how to pay the bills and put food on the table. This poor response allowed even more anti-vaccine fervor to grow by scapegoating vaccines and public health response instead of the underlying capitalist system that refused a comprehensive public health response that recognized those economic rights. We’ll revisit this idea when we talk about an Economic Bill of Rights later in this essay, but suffice it to say that any defense or support of mandates and public health response here is NOT a defense of the Biden administration but actually a critique of how poorly the Biden administration handled necessary public health policy during a pandemic.
It must be recognized that historical socio-economic disparities, sexism, and racism exists within the US, including its medical system, and therefore some communities and individuals have an understandable mistrust of the medical system in general or vaccines in particular. Some of that mistrust unfortunately has been further enflamed by right-wing-funded misinformation campaigns which have often misrepresented how these requirements work, how the vaccines themselves work, and just how many people are “for” or “against” such requirements. Mandates are supported by most Americans, including about 60% support by African American and Indigenous people and over 70% of Asian Americans. Medical professionals must take extra care to reach out to all communities to build trust and counteract misinformation as part of public health response.
Covid Treatments
Ideally we would prevent transmission in the first place, but as a secondary layer we encourage vaccines. As a tertiary layer, if you end up ill, treatments do exist, but there are important caveats and points to make as well as more misinformation.
Paxlovid and monoclonal antibodies have been shown effective at reducing severity and length of symptoms, and modestly lowering the risk of developing Long Covid. However, both treatments are becoming less effective as the pandemic rages on — both Paxlovid and monoclonal antibodies are less effective against newer Omicron Covid variants, and there is concern that variants are developing resistance to antivirals. Paxlovid may also interact with certain drugs and cause side effects, meaning it isn’t right for everyone. Evushield recently had its FDA approval removed as it has lost its effectiveness against new variants. And of course, this is all limited by cost/finances/insurance (more on this below). So while there are treatments, they are growing less effective over time, meaning the need to prevent transmission is growing.
At the start of the pandemic, some had claimed that high-dose Ivermectin would help with Covid infection. Studies have concluded that ivermectin is not effective at reducing viral load. Studies found it generally safe to take, but it won’t do much to help you recover from Covid. Other options that have been clinically shown effective should be used instead.
“Vaccines-Plus” Needs an Economic Bill of Rights
The Delphi consensus is a new multinational consensus between hundreds of medical professionals that promotes a “Vaccines-Plus” strategy to address the pandemic. In other words, the international medical community strongly agrees that the best way to tackle to the pandemic from this point on is to emphasize the need for vaccines, PLUS testing, masking, clean air, and other mitigations. A vaccine only approach is insufficient to keep up with how rapidly Covid is mutating while it transmits freely; vaccine research must continue (and be made available globally by lifting vaccine patents!) while we slow transmission and mutation and “flatten the curve”.
Unfortunately, the Biden administration has quickly winded down all of these actions, even vaccines at this point, as Biden has done very little to promote the new bivalent boosters resulting in only about one in ten having the bivalent booster so far. Vaccine research funding was not renewed by the Democratic-majority Congress and unlikely to be renewed under Republican control. The free Covid test program funding is also running out with no renewal (and honestly I’m not sure how many people were even aware they could apply online to get free tests), and there has been very little talk of Covid being airborne and the need to filter the air and wear masks.
As public health protections are winding back under the political duopoly, we see the consequence of wealth inequality — the wealthy can afford treatment and time off work if they get sick, while the poor are most impacted without access to healthcare or time off work to recover. Wealth inequality is at highs not seen since the Gilded Age; that inequality is worsening with rampant inflation and huge personal debts for things like healthcare (which of course means, as a country without a universal healthcare system, the pandemic is driving many Americans into poverty).
Hospitals are overwhelmed, with doctors and nurses quitting from exhaustion and lack of community support. From an article in The Atlantic entitled “What COVID Hospitalization Numbers Are Missing”: “Biden’s strategy overlooks a crucial truth: The health-care system is still in crisis mode. The ordeals of the past two years have tipped the system—and its people—into a chronic, cumulative state of overload that does not fully abate in the moments of respite between COVID waves.” We don’t know how long the symptoms will persist; there has not been much research into Long Covid for children yet, so many unknowns. Adults with Long Covid already are saying they “don’t know how much more [they] can take” due to the combination of symptoms and lack of treatment or public protections in the US health insurance system.
The US has so failed at containing the virus that while other countries are recovering, the US’s life expectancy continues to drop, a sign that Covid is causing significant death and disability among the US population. A recent study shows that over 250,000 children in the US have lost at least one primary caregiver due to Covid, which, besides the tragedy of losing a parent or other loved one in the first place, means that childcare, schools, and other services will be strained even more. The Omicron variants have hit Black communities the hardest because of systemic inequality and racism; studies show that excess mortality due to Covid disproportionately affects Black communities.
These problems cannot be solved by individual action, yet that’s the message given by politicians and businesses: “personal responsibility”. It’s a meaningless phrase when all the responsibility is on poor people without resources, while those with resources and power are unaccountable — and made worse by a “back to normal” message that doesn’t even recognize the crisis at all.
We therefore must advocate & demand collective action and governmental responsibility in a number of ways I will briefly cover.
Universal Healthcare
It is meaningless to tell folks to “see their doctor” when many cannot do so because they have neither the insurance coverage nor the funds to pay to see a doctor. We need a public healthcare system to take care of folks facing acute or long-term Covid infection and complications. Minimally, this means an emergency “Medicare for All”-style single payer system, in which Medicare covers the costs so that everyone has insurance coverage without medical debt regardless of financial or employment status. Everyone deserves healthcare as a human right. A Yale study concluded that over 335,000 lives may have been saved if universal healthcare was enacted at the start of the pandemic — at least a third of the people who have died due to Covid.
Medicare for All should be a stepping stone to a fully non-profit public National Health Service as exists in many other countries. A National Health Service would include not only insurance but ensure the hospitals and pharmaceuticals themselves are under public control for the common good rather than corporate profits. Nationally funded, but controlled by local communities to ensure the health system is accountable to the people it serves.
Economic Relief
Folks can’t stay home if they test positive if it risks their job/income and therefore risks their housing. We need federally-guaranteed paid sick leave (in addition to paid family leave & vacation time). We need housing as a human right which means rent control, eviction moratoriums, and public housing. We must end student loan and medical debt. True living wages must be the minimum. Collectively, these policies and more are known as the Economic Bill of Rights, part of the Ecosocialist Green New Deal.
The Ecosocialist Green New Deal also includes plans to rebuild the economy and create jobs for everyone — good green jobs cleaning our air and water rather than fossil fuels that destroy our health and planet. Many of these jobs can utilize the National Defense Act to manufacture PPE like masks, HEPA filters to clean the air, and other pandemic-related items. Manufacture vaccines here, and lift the patents so they can also be manufactured & distributed globally for cheap. To support these new jobs and workers transitioning to these jobs, life-long education including tuition-free college is needed. A national free broadband internet strategy is needed to support both work and education from home.
Disabled folks (increasingly disabled by Covid) still deserve housing, healthcare, etc., so we cannot talk only about workers, but also about folks that may not be able to work traditional jobs or at all. Universal income and other programs can supplement the Economic Bill of Rights to ensure all receive necessary care and support.
What Comes Next?
We must have a “no one left behind” attitude when setting public policy, that all life matters, or I worry about the consequences. In Part 3 of my Covid Big Picture, I will explore long-term consequences of the pandemic and the Left’s response (or lackthereof). There are important lessons I hope we all learn before it is too late.
Author’s Note: Updated August 12, 2023, to add links to Part 3. Updated again January 24, 2024, to add a link to latest study showing vaccination lowers risk of long covid. Updated again July 20, 2024, to add a link to new Harvard study on effectiveness of portable air filters.